Superior vena cava syndrome, acute thrombosis on top of chronic lesion
Affiliations: MD Vascular Surgery, Consultant and lecturer of Vascular Surgery, Ain Shams University, Cairo, Egypt
Superior vena cava (SVC) syndrome is a collection of clinical signs and symptoms resulting from either partial or complete obstruction of blood flow through the SVC. This obstruction is most commonly a result of thrombus formation or tumor infiltration of the vessel wall. The most common signs and symptoms include face or neck swelling, upper-extremity swelling, dyspnea, cough, and dilated chest vein collaterals.
A case report.
This case report discusses a 65-year-old male diagnosed with small cell carcinoma of the lung, who presented with an acute onset of facial and neck puffiness, swelling, and dyspnea while in a supine position, persisting for 2 weeks. A venous duplex ultrasound revealed acute thrombosis of the proximal segment of the right subclavian vein. The patient had a history of Port-Cath insertion for chemotherapy infusion, which was identified as a potential provocative factor. Following an oncology consultation, it was determined that there were no further treatment options available, either chemotherapy or radiotherapy, for the small cell carcinoma, as the patient had completed his chemotherapy regimen.
The initial treatment approach included full-dose anticoagulation, removal of the catheter, head elevation, and computed tomography venography with contrast, which subsequently confirmed the presence of SVC thrombosis.
Following the unsuccessful conservative treatment over 1 week, the patient was scheduled for catheter-directed thrombolysis (CDT).
Intervention steps: Access to the right femoral vein was established initially, after which an attempt was made to advance a guide wire (GW) to the SVC, which was unsuccessful. Subsequently, ultrasound-guided access of the right basilic vein was performed above the cubital fossa. The GW successfully traversed the thrombosed SVC, and was positioned at the inferior vena cava (IVC). Intraoperative angiography confirmed the presence of SVC thrombosis (Figure 1). We initiated catheter-directed thrombolysis (CDT) by infusing 50 cc of acetylase (tPA) at a rate of 2 mg/hour for 24 hours. Following the complete lysis of the SVC thrombosis, we primarily dilated the chronic lesion in the SVC using a high-pressure balloon measuring 10 x 40 mm, followed by dilation with an XXL esophageal balloon measuring 18 mm x 4 cm x 75 cm (Boston Scientific). Stent placement was not deemed necessary (Figure 2).
SVC has cleared angiographically of thrombosis, with no significant stenosis or occlusion. The patient improved dramatically after the operation, the dyspnea was relieved, and facial and neck swelling improved (Figures 3 and 4).
Catheter-directed thrombolysis followed by balloon dilatation has a safe and effective role in the management of SVC syndrome due to acute in-top thrombosis of chronic lesions.
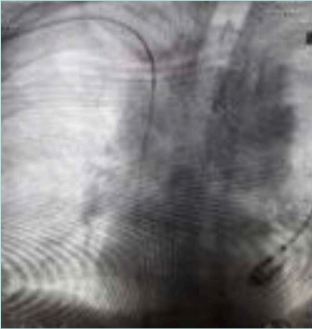
Figure 1. Guidewire pass through superior
vena cava.
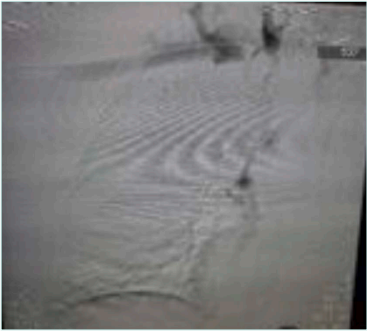
Figure 2. Thrombus load at superior vena cava.
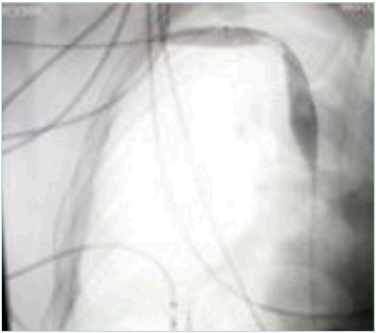
Figure 3. Balloon dilatation for the lesion.

Figure 4. Postdilation angiography.